Advancing healthcare through evidence, innovation, and systems transformation

Value Creation
Delivering Measurable Value in Healthcare
Value in healthcare is defined not by activity, but by outcomes—improved health relative to the cost of achieving it. The organizations that succeed are those that align clinical innovation, operational execution, and financial performance to deliver measurable impact. When care models are designed with this alignment in mind, they not only improve outcomes, but also strengthen resource stewardship, expand access, and drive sustainable growth.
Value Creation in Practice
Value is created when clinical, operational, and financial performance are aligned—not treated as disparate priorities.
1. Improving Outcomes
Designing care models that reduce unnecessary utilization, improve patient outcomes, and enhance the consistency and quality of care delivery.
→ Reduced unnecessary hospitalizations and improved patient outcomes, and enhance the consistency and quality of care delivery.
2. Strengthening Resource Stewardship
Optimizing how care is delivered by reducing inefficiencies, streamlining workflows, and aligning resources to patient need.
→ Reduced workflow redundancies by over 50% and improved resource stewardship
3. Driving Growth and Performance
Translating clinical and operational improvements into measurable business impact—supporting program expansion, contract growth, and revenue performance.
→ Contributed to significant revenue growth, service line expansion, and contract development
Children with Medical Complexity:
Pediatric to Adult Assessment Tool for Home Health (PATHH)
PATHH addresses one of the most significant gaps in pediatric home-based care—creating a standardized, evidence-based framework with the potential to reshape how children with medical complexity are assessed and supported in the home. Developed through a rigorous, multi-phase process, the initiative reflects an undertaking comparable in scale to NICaS, with the long-term goal of informing national care standards for private duty nursing.
Closing the Measurement Gap in Pediatric Home-Based Care
Children with medical complexity (CMC) represent approximately 1% of the U.S. pediatric population, yet account for a disproportionate share of healthcare utilization and cost—including hospitalizations, inpatient days, and total charges. Despite this, care delivery remains heavily weighted toward hospital-based settings, with limited investment in home health services.
This imbalance is sustained in part by the absence of a standardized, psychometrically sound assessment tool capable of objectively communicating the clinical acuity, complexity, and skilled nursing intensity required to safely care for these children in the home. Without such a tool, the expertise of pediatric nurses—particularly those managing technology-dependent children—remains difficult to quantify, limiting visibility to payers, regulators, and utilization management systems.
The Measurement Gap: Why Existing Tools Fall Short
Existing pediatric home health assessment tools are not standardized across states, lack psychometric validation, and are not designed to communicate patient complexity in a way that supports external review and authorization processes.
They fail to capture the full dimensionality of care required for CMC, including:
-
Clinical acuity and diagnostic complexity
-
Technology dependence
-
Functional and developmental status
-
Social determinants of health
-
Family caregiver capacity and health behaviors
-
Cognitive workload of the nurse
-
Time required for direct care and care coordination
In the absence of a comprehensive and validated framework, skilled nursing determinations are often based on incomplete clinical information—contributing to care variability, disparities in access, and avoidable utilization.
Meeting this Critical Need: Developing PATHH
Aveanna Healthcare led the development of the Pediatric to Adult Assessment Tool for Home Health (PATHH)—a standardized, evidence-based instrument designed for the private duty nursing setting and aligned with CMS National Quality Strategy priorities.
PATHH was developed through a rigorous, multi-phase process that included:
-
Systematic review of pediatric literature and clinical best practices
-
Analysis of CMS and multi-state Medicaid guidance
-
Review of authorization tools across more than 40 states
-
A modified Delphi process engaging more than 300 clinical leaders
The framework incorporates a comprehensive, systems-based assessment spanning respiratory, cardiovascular, neurologic, endocrine, mobility, medication, and environmental domains—aligned with nursing scope of practice and informed by both evidence and real-world care delivery.
Validation and Real-World Implementation
PATHH was tested and refined through four phases of field application, progressing from pilot testing to multi-state implementation:
-
Pilot testing with RN clinicians using de-identified cases
-
Expanded testing across broader clinician groups
-
Multi-state deployment involving 200 RNs conducting more than 1,800 patient assessments across 63 locations
-
Final validation including Content Validity Index (CVI) testing, regulatory review, and EMR integration planning
This process resulted in a deployment-ready instrument supported by a multi-year evidence base and a practitioner-informed development model without precedent in the PDN setting.
Summary Illustration of PATHH Development Process

Applied Models at Scale
The following examples illustrate how these principles are applied in complex, real-world healthcare environments.
Population Health Management and NICaS
Older adults living with heart failure, hypertension, and chronic cardiometabolic conditions represent one of the highest-utilization and most clinically vulnerable populations—often experiencing avoidable emergency department visits driven by unrecognized hemodynamic deterioration.
The NICaS (Non-Invasive Cardiac System) enables proactive monitoring through a validated, portable bioimpedance assessment that measures cardiac output, stroke volume, cardiac index, total peripheral resistance, and total body water—without invasive procedures.
Recognizing both the evidence base and the opportunity to extend this capability into home-based care, a comprehensive clinician training program was developed and deployed across CenterWell Home Health locations spanning more than 20 states.
This implementation equipped clinicians with the skills to perform consistent, high-fidelity assessments in the home and communicate findings to physicians through structured protocols—bringing hospital-level insight into the home environment.
The result was a scalable, physician-integrated model for proactive population health management—translating validated technology into measurable reductions in avoidable emergency department utilization and acute hospitalization.
Optimizing Care Delivery
Gentiva and Kindred contributed toward the lead innovation and transformation efforts that aimed to optimize care delivery effectiveness and efficiency for one of the nation’s preeminent Home Health and Hospice providers.

Transitions
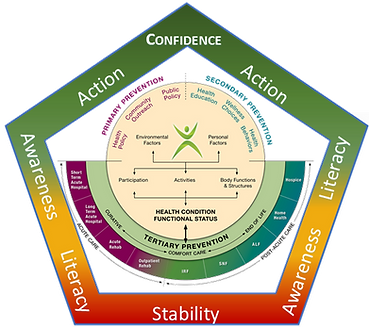
Gentiva and university colleagues collaborated to develop a Wholistic Care Planning Model that incorporated the International Classification of Functioning and Disability (ICF) and accounted for the J-curve phenomenon commonly observed among older adult populations who present with chronic conditions and/or multi-morbidity.
Resource Stewardship

The Kindred at Home (KAH) and university colleagues teamed up to translate successive data analyses into a resource stewardship model that equips clinicians to optimize intervention effectiveness and improve care delivery efficiency via improved prioritization of patient needs and evidence-aligned orchestration of intra/interdisciplinary intervention pacing/spacing.
Comprehensive Perspective
Kindred at Home teammates cross referenced information from Center for Medicare and Medicaid Services with claims data and scientific publications to develop an adaptable, positive health behavior framework that was readily applied across primary, secondary and tertiary spectrums of the healthcare care continuum.